

Dr Abubaker Qutieshat




Profile
- Biography
- Personal Statement
- Scholarly Works
- Research Interest
- Ongoing Research
- Teaching Philosophy
- Research/teaching tools and/or strategies
- Hobbies & extracurricular interests
- Student Testimonials
- Associate Faculty Status, University of Dundee, UK
- Postdoctoral Fellowship, Dundee Dental School, UK
- PhD Restorative Dentistry, University of Dundee, UK
- Clinical Attachment – Restorative Dentistry, NHS Tayside, Dundee Dental Hospital, UK
- Good Clinical Practice (GCP) Certificate - National Institute for Health Research (NIHR), UK
- Medical Education Certificate, Centre of Medical Education, University of Dundee, UK
- NHS Clinical Training and Teaching Certificate, NHS (National Health Service) Scotland, UK
- MSc Conservative Dentistry and Endodontics (Distinction), Jordan University of Science & Technology, Jordan
- Bachelor of Dental Surgery, University of Jordan, Jordan
Multidisciplinary researcher and student-focused academic with more than ten years of experience in Scholarship of Teaching & Learning. Proven experience in leading collaborative research projects, developing curricula, and implementing blended learning in clinical settings.
Committed to the development of students as independent learners and critical thinkers. Operational knowledge of clinical assessment, day-to-day clinical assessment, and structured student feedback.
Granted an honorary research fellowship at the University of Dundee - UK. Possess strong quantitative and qualitative research skills with an established track-record of publications in top scientific journals. Instrumental in leading research teams, training researchers and teaching students at the graduate and undergraduate level in interdisciplinary programs.
Possess strong programming and 3D modelling skills with a track-record of designing and building assistive technologies with a practical value for educators and clinical researchers. Developer of DentAlign software - The first open-source dental 3D alignment tool. Developed and maintained excellent relationships with world-leading research scientists, e-learning specialists, and EdTech entrepreneurs. Forward-thinking and proactive in addressing the needs of vulnerable students.
|
2021 |
|
|
2021 |
|
|
2021 |
|
|
2020 |
|
|
2020 |
|
|
2020 |
|
|
2019 |
|
|
2019 |
|
|
2019 |
|
|
2018 |
|
|
2018 |
|
|
2018 |
|
|
2018 |
|
|
2018 |
|
|
2015 |
Dental Education
Over the last few years, I have been exploring ways to develop and incorporate meaningful relationships between students and faculty members to transform the learning experience. I have developed several instructional methods that recognized students as legitimate knowers and knowledge producers. As an instructor and course coordinator for several courses, I have partnered with undergraduate students as co-instructors in classes, co-coaches in scientific debates, co-researchers in interdisciplinary research projects, and co-authors in published papers.
One of my recent contributions to the dental curriculum was basically an attempt to explore the potential of a new instructional method that integrates ‘debate’ as a teaching tool. This new teaching method was implemented into a single academic semester of an undergraduate conservative dentistry program. I sought to combine knowledge delivery with high-level debate between student debaters, and with the active participation of the audience who were themselves students. This carefully tailored 10-week format ensured good student responsiveness and engaged the entire class in an interactive, participatory setup and proved to be very effective in evidence-based teaching by promoting a deeper approach to learning that can help students develop their self-confidence and enhance their critical thinking skills. This teaching experience has progressed to publication [Med Sci Educator, 29, 181–187 (2019)].
Figure. Research paper that describes the implementation of ‘debate’ as an adjunctive tool in teaching. It was published in Medical Science Educator Journal with three undergraduate students as co-authors.
I have also managed to introduce ‘blended learning’ with a flipped classroom setup for the teaching of a clinical dental course. This course was a 28-week course (7 credit hours) in a curriculum that included one hour lecture and three hours clinic. My implementation of the blended learning model in dental clinical settings was successful based on student academic performance measures and Likert-scale perceptions. Further, the blended learning cohort demonstrated a strong correlation between active online
participation and the overall course grade. This teaching experience has progressed to publication [J Dent Educ, 84, 135-142 (2020)].
Figure. Research paper that describes the impact of ‘blended learning’ on students’ performance in clinical education. The instruction method relied heavily on a discussion forum with students as knowledge builders and fact checkers.
More recently and in collaboration with an interdisciplinary research team, combining psychology and dental education, we investigated the effect of personality traits and brain laterality on the manual
dexterity of the non-dominant hand in pre-clinical operative dentistry training [Eur J Dent Educ, 00, 1-8 (2020)]. This work introduced a new concept in clinical training that has never been reported in any paper
– Symmetrization. The work also proposed a symmetrization-skill-acquisition framework, within the pre-clinical instruction process, which may have a practical and efficient value for the profession of dentistry. The ideal format would be to allow students to assess their needs for optional training and to participate as much, or as little, as they determine necessary.

Figure. Based on the findings of my recent research on the links between laterality, personality and the manual dexterity of the non-dominant hand, the most effective method by which to acquire skills in a complex task is deliberate practice.
During the pandemic lockdown period, I have developed a 3D alignment tool, DentAlign, for the assessment of clinical competence using Java Script language. The tool will be of particular interest to dental instructors. Basically, STL images obtained from any CAD/CAM scanner can be aligned against a reference STL image using an Iterative Closest Point (ICP) algorithm. The tool is open source and is available online: cephcad.com/dentalign/ [Eur J Dent Educ, 25, 397-404 (2021)].

Figure. A, Prepared and reference tooth STL images loaded using the custom software. B, The initial registration was performed by selecting feature points (eg cusp tips) for both images. C, The models were aligned using rigid body transformation (ie Singular Value Decomposition [SVD] technique). D, Point‐based registration was performed with an ICP algorithm. E, Measuring the 3D Euclidean distances between the closest surface points on the two images, with the area of concern being selected before running the algorithm. F, The differences between the two images were evaluated using colour‐mapping methods
Dental Biomaterials
My research in the past several years has focused on applied oral biology, oral physiology, and dental biomaterials beginning with developing a realistic in vitro testing environment and moving more recently to investigating the bioactivity of graphene-based nano-additives to calcium-based cements. By combining machine learning, python coding and virtual simulation, I developed and validated a realistic artificial mouth model for dental research purposes. This innovative creation has received recognition from a top European dental body, the European Federation of Preventive Dentistry, for its pioneering impact on dental research and for its potential application in testing dental therapeutic and preventive agents. The manuscript that described the model received recognition from Wiley publishers, as one of the most downloaded amongst articles published between January 2017 and December 2018 [Clin Exp Dent Res, 4, 105-12 (2018)]. It has also been highlighted in the Scottish Dental Magazine [Scottish Dent Magazine, Mar 2016].

Figure. This paper describes the design, build and validation of a novel artificial mouth 'SALTUS' for dental research purposes. SALTUS is the first artificial mouth model that simulates natural human drinking behavior. This may prove useful to other researchers in diverse fields within and outwith dentistry.
Further and in collaboration with an interdisciplinary research team combining oral biology, oral physiology and dental materials science we were the first to observe real-life oral physiological behavior in a social atmosphere [J Dent, 43, 1352-7 (2015)]. Data representing human physiological behavior was then copied to our in vitro simulation model which in turn led to a paradigm shift in in vitro testing of dental substrates in UOD’s Dental Materials Laboratory.
Figure. Several human physiological values were reported in this experiment and these in turn facilitated the development of the first 'intelligent' artificial mouth model for dental research purposes. A working prototype is currently being used in the dental materials laboratory of Prof. Graham Chadwick at the University of Dundee.
Now that the stage has been set for further progress in the field of biomaterials testing, I am investigating the effect of incorporating bioactive additions into restorative materials at the cell and microbiology laboratory of the University of Dundee. I have previously explored the effects of bioactive additions on the physical properties of glass polyalkenoate cement which led to our proposed chairside methodology of mixing conventional glass ionomer with Collagen type I and RGD peptides (Arg-Gly-Asp) for superior biocompatibility and physico-mechanical reinforcement [J Osseointegr, 11, 497-503 (2019)]. Later, I have worked on a hugely funded research project that aimed at developing a novel nano-reinforced cement-based material and assess its potential for dental application. The preliminary results were outstandingly good, strongly supporting further investigations [J Conserv Dent, 22, 249-54 (2019)]. Just recently, I published a paper describing the effect of modifying a calcium-based cement using graphene oxide nanoplatelets which also sought to determine the optimal concentration (wt %) of nanoparticles that can produce the best nano-modified calcium-based cement formulation [J Conserv Dent, 23, 15-20 (2020)].
I established my independent research program back in 2019, where I managed to secure a fund of £70,000 for a research project that aimed at developing a novel nano-reinforced cement-based material to be used in restorative dentistry. A major aspect of the project was the formulation of a bioactive, nano-reinforced material that can be tailored to the needs of the intended clinical application in terms of setting time, hydration kinetics, antimicrobial spectrum, bioactivity and mechanical properties. My published preliminary results paved the way for an interdisciplinary collaborative relationship between Jordan University of Science and Technology and Dundee Dental School namely the Cell & Molecular Biology lab of Dr. Ian Ellis and Dr. Mohammed Islam.
Throughout my time as a postdoctoral fellow, I have been fortunate enough to be trained on how to utilize artificial intelligence, machine learning, coding, and virtual simulation in the laboratory to improve in vitro conditions providing a more realistic environment for dental researchers. I focused on copying human physiological behavior as closely as possible to an in vitro simulation model. As my technical knowledge and coding skills grew stronger, I designed and developed an innovative smart Arduino-based assistive technology ideal for use in laboratory teaching for the visually impaired learners. I came up with this idea in 2015 when I realized we have this enormous deficiency in our laboratories when it comes to dealing with visually impaired students. This innovative technology is a blend of Python coding, smart sensors, and microprocessors. The first working prototype was described in an article published in 2019 [J Chem Educ, 96, 2333–8 (2019)]. I also focused on formulating an artificial Saliva recipe that best mimics human saliva and its kinematic behavior, which was acknowledged by a pioneer in the field, Prof. Brian Darvell – University of Birmingham.
Figure. Dubbed as a ‘cool tool’ by the Journal of Chemical Education, ‘Design-Bee’ is a smart Arduino-based pH sensor that can be assembled for less than $40, ideal for use in laboratory teaching for the visually impaired learners. We came up with this idea 5 years ago while fooling around with microchips and sensors in the dental materials lab at the University of Dundee, but it only came to light recently! This innovative technology is a beautiful blend of Python coding and sensing robotics in a minimalistic package that makes it a one-of-a-kind achievement.
I will be committed to promote an interdisciplinary approach and work at the interface of Pre- and Paraclinical Dental Sciences across my research projects. I will also work to strengthen the cooperation among faculty members and researchers within and outwith ODC with particular reference to oral epidemiological research, dental care trends, and perceptions of oral health, as evident from the research themes presented in the recently launched Research Action Plan 2021-2023.
As an associate member of staff and an honorary researcher in the Dental Materials laboratory at the University of Dundee, I have an active research agenda that continue to use insights from human behaviour and physiology to develop optimal in vitro environments for the testing of dental substrates and biomaterials and investigate the cellular response of fibroblastic cell lines to bio-ceramics and calcium silicate-based cements in vitro.
Earlier in my academic career I was influenced by Gagne’s theory of instruction as well as Peyton’s model of procedural skills acquisition. Currently I am very much influenced by the concept of students as partners. During the past three years, I have focused on incorporating students as contributors to curricular and pedagogical design, decision-making, implementation, investigation, and analysis.
I have published several works that showcased what students and faculty can do together to further common educational goals. Now I have a strong belief that student–faculty partnership can inspire students to take responsibility for leading the pedagogical process especially if the partnership itself was underpinned by principles of respect, reciprocity, and shared responsibility. My philosophy in teaching is also based on the belief that students have unique strengths and potentials. They only need a push to bring those potentials forward. I always have remarkably high expectations for my students; expect the best out of them and, if they sense that, they will never fail to deliver.
In terms of lesson planning, I mix and match several learning styles and activities. Simply speaking, different students possess different learning styles, on that account, the resultant blend of styles and activities will yield a better learning outcome. I also believe that students’ non-cognitive factors can be used effectively to inform teaching methods and predict academic performance outcomes. Personality traits, for instance, can help inform tailored methods of instruction to better suit vulnerable students may have social, emotional and mental health difficulties and require support. As an introvert myself, I know they can put their ‘extroverted’ faces on if need be. Students just need a bit of support and a friendly learning environment that is grounded in trusting and respectful student-faculty relationships.
In terms of lecture content, I keep relating current material content to other course topics and referring to knowledge gained from previous lectures at several points throughout the lecture. Moreover, I apply the new learning material to students’ real-life experience by providing meaningful examples and scenarios that are markedly linked to their daily-routine activities and/or future-life goals. From the students’ perspective, for clinical skills training in particular, they know they are not doing this entirely for examination purposes; instead, their main objective would be to master the technique and to overcome the stress associated with it. I encourage students at this point to point out their pre-instruction concerns and areas of ambiguity that, they believe, would need special attention. Hereafter, learning objectives are to be modified accordingly to accustom the points raised by students if any.
Whenever possible, I have involved undergraduate students in research projects as co-researchers and curriculum development activities as co-designers. The combination of these experiences has helped shape my teaching philosophy and get where I am today.
My teaching strategy is based on the notion that discussion promotes the co-construction of shared understanding which, in turn, generates more critical thinking, higher-level reasoning strategies, and greater diversity of interactive responses. Students share their questions and ideas with their peers and instructor. They also have the opportunity to get exposed to what other students find difficult to interpret. These perspectives would possibly reconstruct students’ knowledge and reshape their ideas to more fully understand the course material.
I am especially interested in implementing new adjunctive teaching strategies to assist students on how to better grasp the skills that are required to practice as professionals. These included: Q&A discussion
forums, interactive sessions, and crossword puzzles.
Q&A Discussion Forums
Students were encouraged to use the internet-based Q&A discussion forum that was embedded in the course’s original forum (via ProBoards) to extend the interactive discussion and learning activities beyond the class. It was structured to be accessible only to students enrolled in the course and the course instructor. Students posted discussion questions taken from the issues that arose in the clinics, interactive sessions and from the assigned article readings. They were incited to integrate their learning from all instructor-student discussion entries within the discussion forum postings. The instructor’s role was to provide relevant additional material (i.e. drawings, images and article cut-outs), moderate the discussions, and provide feedback to the students. The Q&A discussion forum was aimed at clarifying clinically ambiguous cases and difficult concepts arising from clinical encounters with real patients or the module material itself. The Q&A element was carefully planned and meticulously implemented such that no pending question gets ignored or delayed awaiting a response from the course instructor. This was executed via a notification service using an android app in a cell phone that notified the course instructor
of any new posts to the forum.
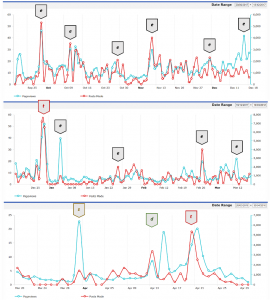
Figure. Q&A forum statistics showing the number of online active students (e: e-lecture release, t: exam, s: clinical work results, d: submission deadline).
Interactive Sessions
The interactive sessions were 1-h sessions that allowed students to apply and integrate the concepts presented in the lectures. The interactive sessions included open discussions, anonymous voting as well as participatory visualization techniques (brainstorming, critical appraisal, and justification of different treatment modalities). Students were presented with a series of clinical scenarios and brief cases (images and/or radiographs) and asked to propose the best treatment option. Moreover, patient role-playing and audience response system questions were used to stimulate students to apply fundamental principles to clinical scenarios. Throughout the interactive session a stylus-enabled tablet connected to a projector was used to deliver hand-written drawings, sketches, and notes, while simultaneously running a slideshow presentation.
These interactive sessions were prepared beforehand and utilized a slideshow; however, they were not conventional lectures for they relied on students’ interaction and the resulting dynamic generations of arguments and counterarguments. More than 80% of my class routinely attended these interactive sessions. This method has also been used to provide background and supporting information in advance of practical clinical sessions where patients are seen and treated. In this way, students accessing the online material in advance of the clinic are primed with background knowledge in order to carry out the proper treatment.
Crossword Puzzles
Sophomore students are introduced to many new terms and concepts in a short time frame. It is a challenge to provide adequate practice and necessary repetition to reinforce key concepts. Crossword puzzles proved to be as a quick and effective way to reinforce essential concepts and vocabulary. The use of crosswords provided an opportunity to discuss and recall essential concepts, think critically, and collaborate in small groups.
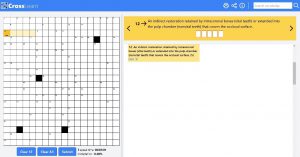
Figure. The use of active learning strategies is recognized as good practice in undergraduate education and is now a widely accepted tool for information delivery and retention
Volunteer Academic Service
Peer reviewer in the following journals:
• Journal of Dental Education
• International Dental Journal
• Frontiers in Education
• Journal of Chemical Education
• HardwareX
• International Journal of Information & Education Technology.
Scientific Outreach and Media appearances
- Scottish Dental Journal. Erosion research wins international award. 2016. Available online.
- Planer PLC. 20 years and going strong. 2016. Available online.
Leadership and Organization
I have organized several charity campaigns, sponsored by Lacalut®, and dedicated to vulnerable and geriatric patients. The charities included free clinical oral examination and treatment planning. Patients also received free medical samples of toothbrushes, toothpastes, and denture adhesives.
Supervisory Activities
Throughout my academic career I was responsible for mentoring students in their clinical master’s and higher specialty programs.
Hobbies
Fishing
